Metabolic Cancer Protocol 2026: An Evidence-Based Integrative Framework
The explosion of online integrative oncology content has created two dangerous extremes. On one side sits conventional oncology—highly evidence-backed, yet occasionally lacking personalized lifestyle integration. On the other lies a viral universe of alternative narratives built on oversimplifications, such as the claim that you can "starve" cancer by cutting out carbohydrates.
The future of successful oncology is neither extreme.
The modern paradigm relies on systems-based integrative oncology—a discipline that merges rigorous tumor biology, cancer metabolism, immunometabolism, and microbiome science into evidence-ranked, patient-specific protocols. This is the foundation of the Metabolic Cancer Protocol 2026.
The Core Integrative Principle: Metabolic and lifestyle interventions are not designed to replace conventional oncology. Instead, they widen the therapeutic window. By stacking these evidence-based strategies alongside standard treatments, we can optimize immune surveillance, support metabolic health, and potentially enhance standard care efficacy.
1. Beyond the Warburg Effect: How Cancer Metabolism Actually Works
One of the most persistent viral health claims online is that "cancer is purely a metabolic disease." This concept stems from a misunderstanding of the Warburg Effect, first described in the 1920s by Otto Warburg. He observed that cancer cells preferentially use aerobic glycolysis (glucose fermentation) to generate energy, even when ample oxygen is available to run more efficient cellular pathways.
While modern oncology firmly recognizes metabolic reprogramming as a core hallmark of cancer, the true scientific picture is far more complex than the "sugar feeds cancer" narrative.
Tumors do not rely on a single fuel source. Instead, cancer cells aggressively exploit a triad of substrates based on their microenvironment, tumor type, and treatment pressures:
- Glucose: Utilized via accelerated glycolysis to drive rapid cellular proliferation and energy generation.
- Glutamine: An amino acid hijacked to fuel the tricarboxylic acid (TCA) cycle, generating critical biomass (proteins and nucleic acids).
- Lipids (Fatty Acids): Exploited for cell membrane synthesis and to maintain structural integrity during rapid division.
Ultimately, these fuel sources are orchestrated to satisfy three distinct metabolic imperatives: rapid proliferation, biomass synthesis, and redox balance (neutralizing the intense oxidative stress generated by uncontrolled cellular growth).
2. The Myth of "Starving" Cancer: Understanding Metabolic Plasticity
The most dangerous oversimplification in alternative oncology is the belief that a strict ketogenic diet or zero-carbohydrate lifestyle can cleanly starve a tumor into submission. Cellular biology explicitly refutes this as a standalone curative strategy.
Cancer cells possess an evolutionary survival mechanism known as metabolic plasticity—the ability to dynamically shift their metabolic machinery when preferred nutrients are restricted.
When glucose availability drops, adaptable tumors easily pivot. They shift from aerobic glycolysis to oxidative phosphorylation (OXPHOS), scavenge local glutamine, or activate autophagy (breaking down their own non-essential cellular components to recycle them into raw nutrients).
This adaptive capacity is highly tissue-specific. While glioblastomas and certain triple-negative breast cancer subtypes exhibit more rigid metabolic profiles—potentially making them more vulnerable to target dietary interventions—pancreatic, lung, and melanoma cells are notoriously plastic. Consequently, blanket dietary mandates fail; clinical metabolic management requires tumor-specific metabolic profiling.
3. Immunometabolism: The Intersection of Metabolism and Immunity
A profound breakthrough in modern oncology is immunometabolism—the study of how metabolic factors dictate immune cell behavior within the tumor microenvironment (TME).
Data reveals that tumors intentionally alter local metabolic conditions to paralyze the host immune response:
- Lactate Accumulation: The byproduct of intense cancer glycolysis creates a highly acidic local environment that actively suppresses effector T-cell and Natural Killer (NK) cell functionality.
- Nutrient Competition: Tumors rapidly consume local glucose and tryptophan, effectively depriving infiltrating immune cells of the energy required to execute anti-tumor attacks.
- Macrophage Reprogramming: High concentrations of lactic acid signal tumor-associated macrophages (TAMs) to transition into an immunosuppressive "M2" phenotype, shielding the tumor from immune clearance.
This metabolic hostage-taking explains why patients with identical genetic tumor profiles can experience completely disparate responses to identical immunotherapies. Success relies heavily on the metabolic fitness of the local immune microenvironment.
4. Tumor Microenvironment (TME): The Hidden Battlefield
A tumor is not merely a cluster of rogue cells; it is a complex, living ecosystem termed the tumor microenvironment (TME). The TME consists of cancer cells intertwined with extracellular matrix components, immune cells, blood vessels, and specialized fibroblasts.
The TME coordinates tumor survival through distinct mechanisms:
- Angiogenesis: Directing the growth of new, chaotic blood vessels to supply the tumor with oxygen and systemic nutrients.
- Immune Exclusion: Generating dense physical and chemical stromal barriers that physically prevent therapeutic T-cells from penetrating the core of the tumor.
- Metastatic Priming: Remodeling the local matrix to facilitate cancer cell migration into the bloodstream.
Reshaping the TME through safe, supportive therapies—such as targeted anti-inflammatory strategies and metabolic normalizers—remains a major frontier in maximizing standard treatment outcomes.
5. Diet, Fasting, and Metabolic Therapies: What the Science Supports
Dietary intervention is a primary focus for patients seeking integrative options. Here is what large-scale human data actually confirms regarding nutrition and oncology.
Ultra-Processed Foods (UPFs) and Cancer Survival Outcomes
The clinical connection between ultra-processed food consumption and negative oncological outcomes is clear. A landmark umbrella review in The BMJ encompassing 45 meta-analyses and nearly 10 million participants established a direct correlation between high UPF intake and increased cancer incidence, metabolic dysfunction, and all-cause mortality.
Recent data has strengthened this connection:
- Survivorship Risk: A study in AACR Cancer Epidemiology, Biomarkers & Prevention determined that among long-term cancer survivors, high UPF intake was independently associated with significantly reduced overall survival due to the metabolic stress of excess refined sugars and trans fats.
- Additive Concerns: A large prospective cohort study published in The BMJ (NutriNet-Santé) identified a distinct association between high consumption of common food additive preservatives and elevated rates of breast and overall cancers.
The Impact of Insulin Resistance on Cancer Risk
Insulin resistance acts as a systemic driver of tumor progression. A study published in Nature Communications utilizing machine-learning models demonstrated that elevated insulin resistance correlates with a 25% higher overall cancer risk across 12 distinct cancer types. The data revealed that uterine cancer was the most vulnerable (showing a 134% increased risk), followed closely by liver, pancreatic, and colorectal malignancies. Elevated systemic insulin directly stimulates insulin-like growth factor 1 (IGF-1) receptors on cancer cells, activating the pro-growth PI3K/Akt/mTOR pathway.
Fasting-Mimicking and Ketogenic Protocols
Therapeutic fasting and highly structured ketogenic diets are capable of modifying systemic insulin, lowering IGF-1 levels, reducing mTOR signaling, and elevating circulating ketone bodies (beta-hydroxybutyrate).
However, unsupervised, long-term caloric deprivation introduces significant clinical risk. Unmonitored fasting can accelerate cancer cachexia (muscle wasting) and deplete the amino acid reserves required for robust bone marrow and T-cell production, ultimately weakening anti-tumor immune responses.
The Mediterranean Diet Baseline
For the vast majority of patients, the Mediterranean diet provides the safest, most effective nutritional baseline. Composed of whole vegetables, cruciferous greens, legumes, extra virgin olive oil, wild-caught fish, and moderate nuts, this pattern acts as a powerful anti-inflammatory and insulin-sensitizing framework. It delivers essential micronutrients without risking nutritional deficiencies or dangerous weight loss.
The Systemic Metabolic "Headwind" Model
As synthesized in Nature, the clinical goal of integrative nutrition is to build a systemic metabolic "headwind"—a physiological state that subtly hampers tumor kinetics while optimizing patient vitality.
[ Eliminate UPFs & Additives ] + [ Reverse Insulin Resistance ] + [ Optimize Nutrient Timing ]
│
▼
[ Creates Systemic Metabolic "Headwind" ]
│
▼
Slows Tumor Kinetics & Optimizes Immune Fitness
By removing ultra-processed foods, correcting insulin resistance, and strategically utilizing nutrient timing, we put downward pressure on tumor growth factors without introducing malnutrition.
6. Repurposed Drugs and Natural Compounds in Integrative Oncology
Drug repurposing—the clinical practice of utilizing well-characterized, low-cost medications originally approved for non-oncological conditions—presents an exciting frontier due to established human safety profiles.
Current Clinical and Preclinical Status
While cell-line and animal models display interesting activity, it is vital to categorize these options by true evidence tiers rather than social media hype:
- Metformin: The most rigorously evaluated repurposed agent. It functions by activating AMPK, improving systemic insulin sensitivity, and lowering circulating IGF-1. It is currently undergoing multiple Phase III clinical trials globally.
- Statins & Aspirin: Backed by substantial retrospective epidemiological data indicating a correlation with reduced recurrence rates in colorectal and cardiovascular-adjacent malignancies.
- Mebendazole: Shows interesting preclinical activity in disrupting microtubule synthesis (similar to taxane chemotherapies). Human data is currently limited to Phase I/II safety trials.
- Ivermectin: Preclinical in-vitro models suggest interesting synergistic potential when combined with immune checkpoint inhibitors. However, robust human data remains absent.
Evidence Warning: Data regarding agents like ivermectin or mebendazole remains primarily in the preclinical or early phase stage. Case series and un-peer-reviewed preprints cannot establish clinical efficacy or replace standard medical treatments. Furthermore, certain natural compounds can interact unpredictably with hepatic pathways, potentially altering chemotherapy clearances. All repurposed therapies require direct professional supervision.
7. The Gut Microbiome Revolution in Cancer Care
The understanding of the gut microbiome as a critical determinant of immunotherapy efficacy represents a major milestone in modern oncology.
Landmark Clinical Evidence
Landmark clinical papers published in Science and Nature Medicine demonstrated that the specific taxonomic composition of a patient's gut microbiome directly predicts their response to anti-PD-1/PD-L1 immune checkpoint inhibitors.
Favorable Gut Microbiota (e.g., Akkermansia) ──► Primes Dendritic Cells ──► Enhances CD8+ T-Cell Infiltration
The presence of specific commensal microbes, such as Akkermansia muciniphila and Faecalibacterium prausnitzii, primes peripheral dendritic cells. This priming dramatically enhances the ability of cytotoxic CD8+ T-cells to infiltrate and clear tumors.
Conversely, profound gut dysbiosis increases intestinal permeability, driving systemic endotoxemia and chronic inflammatory signaling that accelerates tumor progression. Notably, studies confirm that the administration of systemic broad-spectrum antibiotics immediately prior to or during immunotherapy correlates with significantly shorter progression-free survival.
References:
- Routy B, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy. Science. 2018;359(6371):91–97.
- Gopalakrishnan V, et al. Gut microbiome modulates response to anti–PD-1 immunotherapy. Science. 2018;359(6371):97–103.
- Zitvogel L, Ma Y, Raoult D, Kroemer G, Gajewski TF. The microbiome in cancer immunotherapy. Nat Rev Immunol. 2018;18(8):521–533.
- Matson V, et al. The commensal microbiome is associated with anti–PD-1 efficacy. Science. 2018;359(6371):104–108.
- Helmink BA, et al. The microbiome, cancer, and cancer therapy. Nat Med. 2019;25(3):377–388.
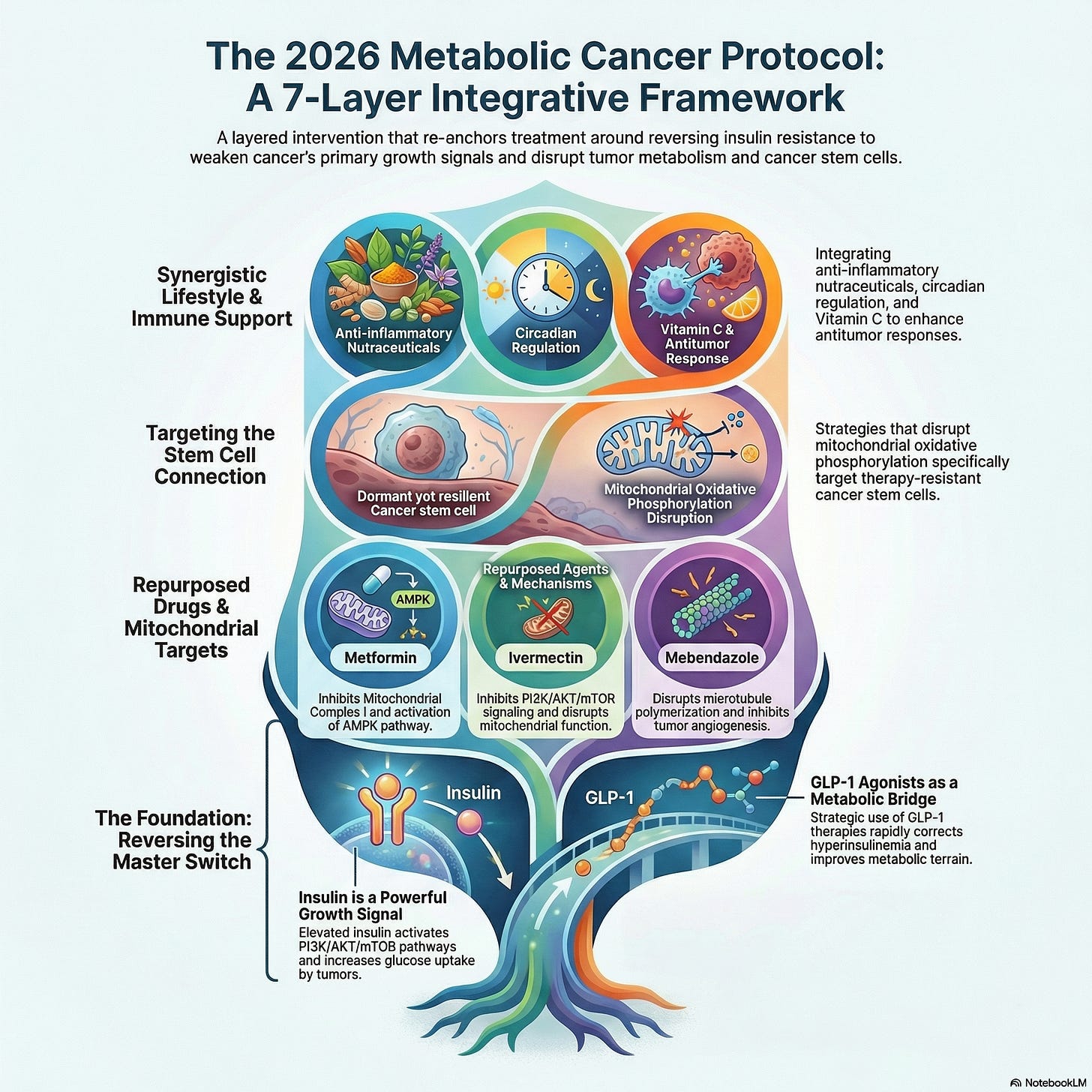
8. The 7-Layer Metabolic Cancer Framework
To synthesize these complex, interacting physiological networks into a clinical strategy, the Metabolic Cancer Protocol 2026 organizes care into a structured, seven-layer systems framework:
- Layer 1: Standard Oncology Integration (Mandatory Core)
Prioritizes standard-of-care interventions (surgery, chemotherapy, radiotherapy, targeted therapy, and immunotherapy) as the non-negotiable therapeutic core. All subsequent layers function strictly to support this foundation. - Layer 2: Immunotherapy & Checkpoint Optimization
Protects T-cell function within the tumor microenvironment by tracking metabolic metrics, reducing tissue hypoxia, and avoiding unnecessary systemic immunosuppression. - Layer 3: Microbiome Preservation
Enhances immunotherapy response rates by avoiding indiscriminate antibiotic use around treatment cycles, introducing diverse prebiotic fibers, and optimizing gut-barrier integrity. - Layer 4: Insulin Resistance & IGF-1 Eradication
Targets systemic growth drivers by maintaining optimal fasting insulin levels and lowering hemoglobin A1c (HbA1c) through targeted exercise and metabolic therapies. - Layer 5: Precision Dietary Restructuring
Establishes an anti-inflammatory, micronutrient-dense foundation by removing ultra-processed foods, refined carbohydrates, and chemical preservatives. - Layer 6: Oncologist-Guided Repurposed Therapies
Evaluates well-studied, low-risk repurposed metabolic agents (such as Metformin) based on the patient's unique metabolic labs and tumor type. - Layer 7: Systemic Inflammation Mitigation
Monitors and downregulates inflammatory biomarkers (like High-Sensitivity C-Reactive Protein and Interleukin-6) through targeted lifestyle interventions, continuous sleep optimization, and structured stress resilience strategies.
Final Evidence Verdict: What Works vs. What Lacks Data
Tier 1: High Validation (Phase III Trials / Large Human Cohorts)
- Supported Interventions: Standard Oncology Care, Ultra-Processed Food (UPF) & Chemical Additive Elimination, Systemic Insulin Resistance Management, and a Mediterranean Dietary Base.
- Core Scientific Rationale: Multi-million participant epidemiologic datasets and umbrella reviews establish undisputed, direct links between highly processed diets, chronic hyperinsulinemia, and significantly reduced overall survival across multiple solid tumor types.
Tier 2: Moderate Validation (Phase I/II Trials / Mechanistic Human Data)
- Supported Interventions: Targeted Gut Microbiome Engineering, Adjuvant Metformin Therapy, and Clinician-Monitored Fasting-Mimicking Diets.
- Core Scientific Rationale: Highly reproducible clinical trial data confirms that specific baseline gut microbiome signatures directly predict checkpoint inhibitor success. Concurrently, Metformin effectively lowers circulating insulin and downstream growth pathway signaling in phase II environments.
Tier 3: Preclinical Status (Cell Cultures / Animal Models Only)
- Supported Interventions: Mebendazole Protocols, Ivermectin-Immunotherapy Combinations, and High-Dose Isolated Botanical Compounds (e.g., Curcumin extracts).
- Core Scientific Rationale: These agents display compelling anti-proliferative or synergistic mechanism pathways in vitro (in laboratory cell lines), but currently lack completed, randomized controlled trial evidence in human oncology.
Frequently Asked Questions
Can you cure cancer by cutting out sugar?
No. While reducing refined sugar is crucial for lowering systemic insulin and systemic inflammation, cancer cells possess high metabolic plasticity. If glucose is entirely removed, tumors readily adapt by utilizing alternative fuels like glutamine, fatty acids, or internal cellular recycling.
Does the ketogenic diet work for all types of cancer?
No. The ketogenic diet is highly context-dependent. Preclinical data suggests it may be helpful as an adjunct for specific tumors with low metabolic flexibility, such as certain glioblastomas. However, for other adaptable or lipid-dependent cancers, a ketogenic approach can be ineffective or even counterproductive.
Why is antibiotic use discouraged during immunotherapy?
Broad-spectrum antibiotics can deplete beneficial gut microbiota species like Akkermansia muciniphila. These specific bacteria are required to prime and activate the immune cells that allow checkpoint inhibitors to recognize and destroy cancer cells.
Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. The Metabolic Cancer Protocol 2026 represents an integrative framework for discussion. All dietary, lifestyle, or repurposed drug interventions must be reviewed, authorized, and monitored by a qualified oncologist within a professional clinical setting.

.png)
Comments
Post a Comment